

Abstract
Background and objective. An important proportion of patients with polycythemia vera (PV) and essential thrombocythemia (ET) are diagnosed in the seventh and eighth decades of life. Because of the chronic course of PV and ET and the advanced age of patients, many will actually die from age-related ailments instead of the myeloproliferative neoplasm, so the disease's impact on life-expectancy remains largely unknown. This registry‐based study was aimed at investigating the excess mortality attributable to PV and ET in a large series of patients diagnosed and managed according to modern criteria.
Methods. We queried the databases of the Spanish Group for Chronic Myeloproliferative Neoplasms (GEMFIN) to retrieve patients diagnosed with PV or ET after 1980. Criteria for diagnosis and treatment modalities were the internationally recommended ones in each period.
Excess mortality was defined as the complementary of the ratio between the actuarial survival observed in the cohort of patients and the expected survival derived from the general Spanish population matched to the patients by age, sex, and calendar year at diagnosis, and was estimated by the Dickman's method (Stat Med 2004;23:51). Spanish life-tables stratified by age, sex, and calendar year were obtained from the Human Mortality Database (www.mortality.org).
Results. A total of 3,268 patients were included in the study (PV: 1,731; ET: 1,537). Median age (interquartile range) and sex distribution in the PV and ET groups were 67 (55-75) years, 48% females, and 62 (48-74) years, 61% females, respectively. At the study closing date, 270 (16%) patients with PV and 202 (13%) with ET had died. Estimated median survival was 20.2 years for PV patients and 23.8 years for ET patients. Transformation into acute myeloid leukemia/myelodysplastic syndrome was diagnosed in 76 (4.4%) patients with PV and 63 (4.1%) with ET. Three hundred and seventy-one patients (170 ET, 201 PV) had one or more episodes of thrombosis over the course of the disease.
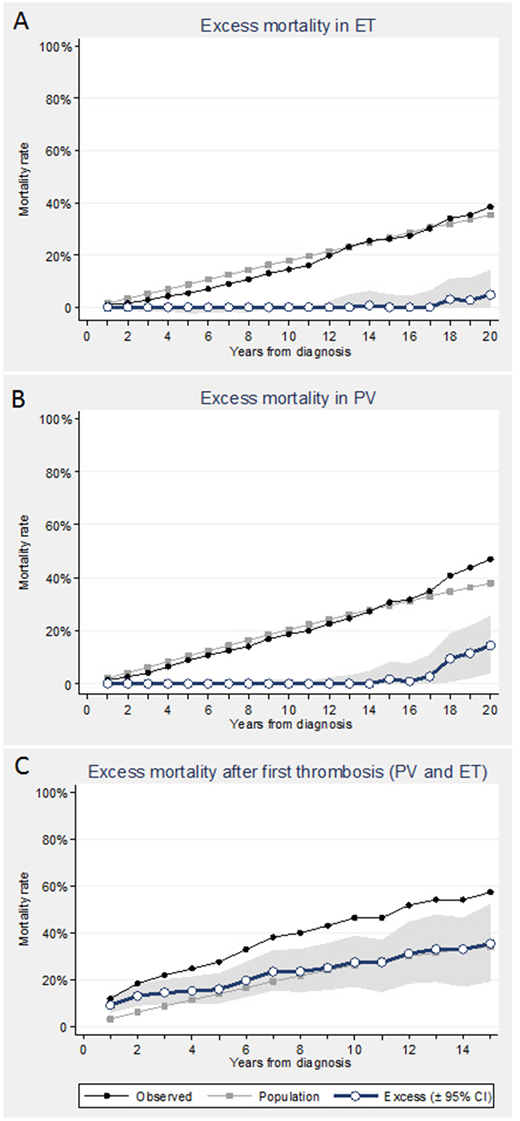
No significant excess mortality attributable to ET was detected at 20 years from diagnosis (figure 1a). In PV, mortality did not significantly deviate from matched general population until 18 years from diagnosis (figure 1b). In both diseases, excess mortality significantly increased after the first recorded thrombotic event (figure 1c).
Conclusion. From the population viewpoint, ET and PV do not carry an increased excess mortality until late in the second follow-up decade or later. Nevertheless, appearance of a thrombotic event significantly increases the subsequent excess mortality.
Hernandez Boluda:Incyte: Consultancy; Novartis: Consultancy. Ferrer Marin:Novartis: Consultancy, Research Funding; Incyte: Consultancy. Gómez-Casares:Bristol-Myers Squibb: Speakers Bureau; Incyte: Speakers Bureau; Novartis: Speakers Bureau. Cervantes:Celgene: Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Hospital Clinic Barcelona: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal